covid19_science
Table of Contents
COVID-19 science
see also:
Introduction
- Covid-19 is a viral pandemic caused by the pathogen SARS-CoV-2 which belongs to the coronaviridae / corona viruses (CoV)
- It originated in Wuhan in China with 1st cases recognized in Dec 2019
- it is thought to have evolved from a coronavirus in bats
- it shares 96.2% identity at the nucleotide level with the coronavirus RaTG13, which was detected in horseshoe bats (Rhinolophus spp) in Yunnan province in 2013 1)
- this virus appears to be unique amongst primary respiratory viruses in that it is a respiratory virus that can infect vascular enothelial cells throughout the body
The SARS-CoV-2 virus
- it is a spherical enveloped RNA virus of around 0.1 micron in diameter and being enveloped, this means it does not require host cell lysis to spread but it could replicate within the host cell and be secreted through usual cell processes and thus this could allow infectivity in the pre-syptomatic phase.2)
- the virus surface has spike proteins which allow the virus to bind to ACE2 proteins on host cells and activate a cellular mechanism to enter the cell where it can replicate
- viral replication
- as it is a virus it cannot replicate without being inside a host cell
- CoVs employ a multi-subunit replication/transcription machinery.
- A set of non-structural proteins (nsp) produced as cleavage products of the ORF1a and ORF1ab viral polyproteins assemble to facilitate viral replication and transcription.
- A key component, the RNA-dependent RNA polymerase (RdRp, also known as nsp12), catalyzes the synthesis of viral RNA and thus plays a central role in the replication and transcription cycle of COVID-19 virus, possibly with the assistance of nsp7 and nsp8 as co-factors3)
- disruption of host cell protein synthesis and the innate immune response:
- one end of the Nsp1 protein produced by SARS-CoV-2 interacts with the 40S subunit in such a way that it prevents binding of the mRNA and inhibits the formation of functional ribosomes and can also interact with specific configurational states of the fully assembled ribosome. The shutdown of protein synthesis leads to an almost complete collapse of the innate immune response by inhibiting a vital signaling cascade.4)
Major variants of concern or monitoring
- Nov 2025: Australia is seeing a mixture of the subvariants NB.1.8.1, PQ.17, PE.1.4, RE.1.1, and increasingly commonly, LP.8.1. Aust. TGA has registered Pfizer’s LP.8.1 vaccine, designed specifically to target the spike protein of LP.8.1
- XFG
- a recombinant of LF.7 and LP.8.1.2, is growing globally and predominates in Europe in mid 2025
- NB.1.8.1
- 1st detected Jan 2025; along with XFG, it is a descendant of the BA.2.86 (Pirola) COVID-19 variant
- NB.1.8.1 developed a spike mutation pattern nearly identical to that of XEC.25.1, another highly immune-evasive Omicron subvariant, but did so through a separate evolutionary path.5)
- May 2025 - cases surging globally; 40% of cases in Vic, 25% of cases in WA/NSW, 20% of cases in Qld;
- in Hong Kong, surged from virtually zero to nearly 90% of all sequenced SARS-CoV-2 cases in just two months and by late March had become the dominant strain
- estimated to have a ~120% weekly growth advantage over other circulating variants, allowing it to rapidly overtake the previously dominant LP.8.1 lineage.
- LP.8.1
- 1st detected July 2024; descended from Omicron KP.1.1.3 which descended from JN.1
- has mutations at six locations in its spike protein including V445R which seems to make it more transmissible and more readily bound to human lung cells
- in March 2025 was accounting for 20% of cases in NSW and 60% of cases in the UK
- XEC
- 1st detected in Germany in Aug 2024
- the product of a recombination (exchanged pieces of genetic material between two variants) between the KS.1.1 variant and the KP.3.3 variant. These two parent variants are closely related, having both evolved from JN.1
- has the relatively rare T22N mutation (inherited from KS.1.1) combined with Q493E (from KP.3.3) in the spike protein
- became the dominant strain in Australia late 2024-early 2025
- JN.1 lineage “FLiRT”
- May 2024, United States, FLiRT has quickly overtaken JN.1 as the dominant strain
- KP.1 and KP.2 - additional mutations in the spike protein of these variants typically seen at R346T, F456L and V1104L
- Sept 2024:
- KP.3.11 is most dominant strain in Europe and Nth America
- KP.3.3 dominates Asia
- more transmissible than previous iterations of the coronavirus but usually causes less severe illness
- BA.2.86 lineage “Pirola”
- 1st reported in Denmark in August 2023
- has many unique mutations (at least 30 in the spike protein, thus is is highly capable of evading the pre-existing anti-SARS-CoV-2 immunity) and is phylogenetically distinct from the currently circulating Omicron XBB lineages
- JN.1 (BA.2.86.1.1) emerged in Dec 2023 in Japan and USA contains a hallmark mutation L455S in the spike protein (giving increased viral transmissibility and immune evasion ability) and three other mutations in the non-spike proteins. 6)
- responsible for nearly all cases in Australia in 1st half of 2024
- Omicron XBB
- main variant causing illness in Australia in 2023:
- the F456L mutation that led to the rise of EG.5.1, also known as Eris
- more recently, paired “FLip” mutations F456L+L455F
- Omicron
- initially identified in Sth Africa and started spreading globally in Nov 2021
- many more mutations including to spike protein raises concerns it may not only be more contagious but may may be able to evade current vaccines
- appears to have 3-8x risk of reinfection compared with Delta
- 20-40x reduction in neutralising activity by Pfizer vaccinee sera and antibodies are 10x less effective than for Delta
- AZ vax even less effective but a mRNA booster appears to result in vaccine effectiveness of 70-75% for mild disease
- in UK in Dec 2021, infections are doubling every 2-3 days with Rt of around 4
- replicates 70 times more quickly than Delta in tissues that line airway passages, which may facilitate person-to-person spread
- replicates 10 times more slowly in lung tissue and to 10x less amount than the original version of the coronavirus, which appears to contribute to less severe illness in terms of lung infection and cytokine storm effects
- this appears to give a less severe infection
- UK data in Dec 2021 suggests it is 50-70% less likely to result in hospitalisation than Delta
- much less likely to cause anosmia and cough while most have headache, fever, sore throat, runny nose, sneezing and fatigue
- Pfizer booster appears to offer 70% protection for symptomatic infection after 2 weeks (cw 90% for Delta) but this wanes to 45% by 10wks, whereas Moderna booster stays at 70% by 10wks7)
- in early 2022, a BA.2 sub-variant increasingly became the dominant variant as its native R0 of approx 12 makes it as contagious as measles.
- the BA.4 and BA.5 variants (1st detected in Sth Africa in Jan 2022 and Feb2022 respectively) became dominant in Australia in May-June 2022 thanks to an R0 of ~18! In addition, they seem to cause more severe illness than earlier Omicron variants
- “BA.2.75” variant arose in India in early May 2022 and has more mutations than BA.5
- C.1.2
- first identified in the Gauteng and Mpumalanga provinces in Sth Africa May 2021;
- main issue is the speed of mutations and number of mutations but it is yet to be seen if it becomes a variant of concern to out-compete with Delta
- Mu variant
- B.1.621 originated in Sth America and was placed as variant of concern by WHO on 30/8/21
- appears to effectively compete with Delta accounting for 39% of Colombia's cases during the Delta surge but global prevalence is decreasing
- Lambda S strain
- belongs to the C.37 VOI lineage and emerged in July 2020
- by July 2021 it was predominantly spreading in South American countries where it seems to be evading vaccination immunity
- the spike protein of the Lambda variant is more infectious and it is attributed to the T76I and L452Q mutations; insertion of RSYLTPGD246- 253N mutation in the NTD of the Lambda Spike protein is associated with the increased virulence and is responsible for evasion from neutralizing antibodies 8)
- Kappa strain (B.1.167.1)
- “Indian strain” from Oct 2020
- said to be 50% more infectious than UK variant and R0 > 6 while transmission period seems to be as short as 24hrs from infection instead of previous 4-7 days
- community spread in Victoria, Australia in April 2021
- Eta strain (B.1.525)
- multiple countries from Dec 2020
- Iota strain (B.1.256)
- USA from Nov 2020
- Theta strain (P3 Philippines)
- Philippines from Jan 2021
- Zeta strain (P2 Brazilian)
- Brazil from Apr 2020
- Epsilon strain (B.1.427/B.1.429)
- USA from Mar 2020
- Delta strain (B.1.167.2)
- from India Oct 2020
- said to be 50% more infectious than UK variant and R0 > 6 while transmission period seems to be as short as 24hrs from infection instead of previous 4-7 days
- NB. an R0 of 6 suggests that herd immunity would occur once more than 84% of entire population (including children) are vaccinated or infected and now immune
- AY.4.2 Delta variant seems to be emerging in UK since Aug 2021 and by Nov 2021 accounted for 10-14% of cases
- 2 main additional mutations:
- A222V was first seen in the B.1.177 lineage in Spain in 2020
- Y145H mutation appears to have increased the transmissibility of the virus by 10-15%
- Gamma strain (P.1 Brazilian strain)
- first identified in Japan among travelers from Brazil in January 2021 but documented earliest from Brazil in Oct 2020
- a branch off the B.1.1.28 lineage
- 17 unique mutations, including three in the receptor binding domain of the spike protein.
- has the N501Y mutation as with UK strain
- has the E484K mutation as with Sth African strain
- seems to have a much higher rate of infection and severe illness in young adults
- 1.4–2.2 times more transmissible and was shown to be capable of evading 25–61% of inherited immunity from previous coronavirus diseases, leading to the possibility of reinfection.
- can be 10–80% more lethal
- Beta strain (B.1.351 South African strain)
- first reported in South Africa in December 2020 but found from May 2020 onwards
- shares some mutations with B.1.1.7 but does not contain the deletion at 69/70
- has multiple mutations in the spike protein, including K417N, E484K, N501Y
- 50% more transmissible than pre-existing variants
- seems to reduce the efficacy of the AstraZeneca vaccine against mild to moderate illness
- neutralisation titres significantly reduced to Pfizer and AstraZeneca vaccines9)
- Alpha strain (B.1.1.7 UK strain)
- first reported in the United Kingdom in December 2020 but found from Sept 2020 onwards
- more transmissible than pre-existing “wild” variants
Transmission
- thought to be primarily via droplet spread hence close proximity or direct contact is important
- lesser roles for aerosol spread (especially if aerosol generating procedures (AGPs) or poorly ventilated rooms) and fomite contact “indirect” spread (esp. bathrooms)
- possible roles for faecal-oral spread (toilet flushing), public urinals and sexual transmission
- a Japanese study estimated that the probability of direct transmission infection is almost 20 times higher indoors compared to outdoors
- catching the virus whilst outdoors appears to be rare and requires close contact (although risk is probably higher if the infected person is exercising), in a Chinese study, only 1 in 314 outbreaks could be traced to outdoor contact
- wearing masks dramatically reduce the numbers of virus particles in the air
- transmission is around 25-53% less in Summer vs Winter in temperate climates in Europe10)
- see also:
75% of droplets observed are moving at velocities less than 0.5 m/s and the motion is equally distributed in all the directions, which implies that they do not settle rapidly and may follow the ambient airflow pattern. These results points toward high aerosol generation, as the behaviour of these droplets is like airborne particles source: Clinical Infectious Diseases Sept 2020. Droplets and Aerosols generated by singing and the risk of COVID-19 for choirs
Viral stability outside of host cells
- virus can survive at least 3 days on most surfaces and is more stable on plastic and stainless steel (median half life of 6.8hrs and 5.6hrs respectively), than on copper and cardboard11)
- viral load in the air and on domestic surfaces in the homes of infected persons appears to be minimal, however, a possibly more significant reservoir of viral particles may be in wash basins, showers and toilets and in the waste water.12)
- Viable virus has been isolated from air samples collected 2 to 4.8m away from patients suggesting aerosol spread in hospitals especially if poorly ventilated13)
- an Australian study suggests for each 1% drop in relative humidity, there was about a 7% increase in the pooled estimate of daily counts of COVID‐19 cases in the NSW 1st wave of community transmission. There was no correlation with outdoor temperatures. 14)
- another Australian study in Oct 202015) showed the virus, in the absence of UV light, can:
- survive up to 28 days on some surfaces at 20degC, 50% RH and in the dark on glass, stainless steel, vinyl and banknotes
- can survive over a week at 30degC
- but survives only up to 24 hours at 40degC on some surfaces
Host cell mechanisms
- the virus binds to the cell's neuropilin-1 receptor and, if present, the ACE2 protein on host cells but requires these cells to also express TMPRSS2 (or perhaps an alternate protein). Two proteins, PIKFyve kinase and CD147 have also been shown to bind Spike protein and facilitate viral entry 16)
- SARS-CoV-2 has a 10-20-fold higher affinity of ACE2 compared to SARS virus17)
- binding of the coronavirus S (spike) protein to ACE2 triggers a conformational change in the S protein of the coronavirus, allowing for proteolytic digestion by host cell proteases (TMPRSS2)
- TMPRSS2 expression and cell fusion pathway appears to overcome the antiviral effect of hydroxychloroquine which blocks the alternate Cathepsin L pathway to fusion with cells, providing a mechanistic explanation for hydroxychloroquine's poor therapeutic efficacy against SARS-CoV-2 – despite somewhat encouraging cell culture results18)
- the intracellular enzyme furin plays an important role in this viral life cycle of SARS-CoV-2 and this is distinctly different than SARS-CoV.19)
- The furin cleavage site in the SARS-CoV-2S protein may provide a priming mechanism, and Alveolar type II cells were strongly positive for furin while transient secretory cells had an intermediate level of expression
- nasal epithelial cells appear to be the primary target for infection as these are more susceptible than lower airway cells to infection, however, the same types of nasal epithelial cells from various human donors vary markedly in their vulnerability to infection plus the virus does not seem to infect other nasal cells such as club cells despite them also expressing both ACE2 and TMPRSS2 which suggests there are other yet to be discovered factors which permit infection20)
- an alternate cellular access to ACE2 binding is binding to the transferrin receptor (TfR) and was then transported into cells - the A529 residue in TfR was essential for interactions with the spike 21)
- After cellular detection of viral entry into a host cell, interferon (IFN) induction of interferon-stimulated genes (ISGs) is essential for host antiviral defense. IFNα also drives up-regulation of ACE2. SARS-CoV-2 could exploit species-specific interferon-driven up-regulation of ACE2, a tissue-protective mediator during lung injury, to enhance infection 22)
- a lung organoid model23) seems to show that when exposed to the virus:
- the virus begins to replicate rapidly, reaching full cellular infection just six hours after infection.
- cells begin to produce interferons – signals to neighbouring cells, telling them to activate their antiviral defences
- after 48 hours, the interferons triggered the innate immune response and the cells started fighting back against infection
- 60 hours after infection, a subset of alveolar cells began to disintegrate, leading to cell death and damage to the lung tissue.
Host cell ACE2 expression
which cells express both ACE2 and TMPRSS2
- the major target cells which express BOTH ACE2 and TMPRSS2 are:
- nasal goblet secretory cells
- nasal ciliated cells
- conjunctival cells
- type II pneumocytes
- upper oesophageal epithelium
- ileal and colonic enterocytes
- in addition, gall bladder and CBD cells also co-express these.
- interestingly, fetal and placental tissues appear not have cells that express ACE2 and TMPRSS2 concurrently except for some medullary thymic epithelial cells. See https://media.springernature.com/full/springer-static/image/art%3A10.1038%2Fs41591-020-0868-6/MediaObjects/41591_2020_868_Fig1_HTML.png?as=webp 24)25)26)
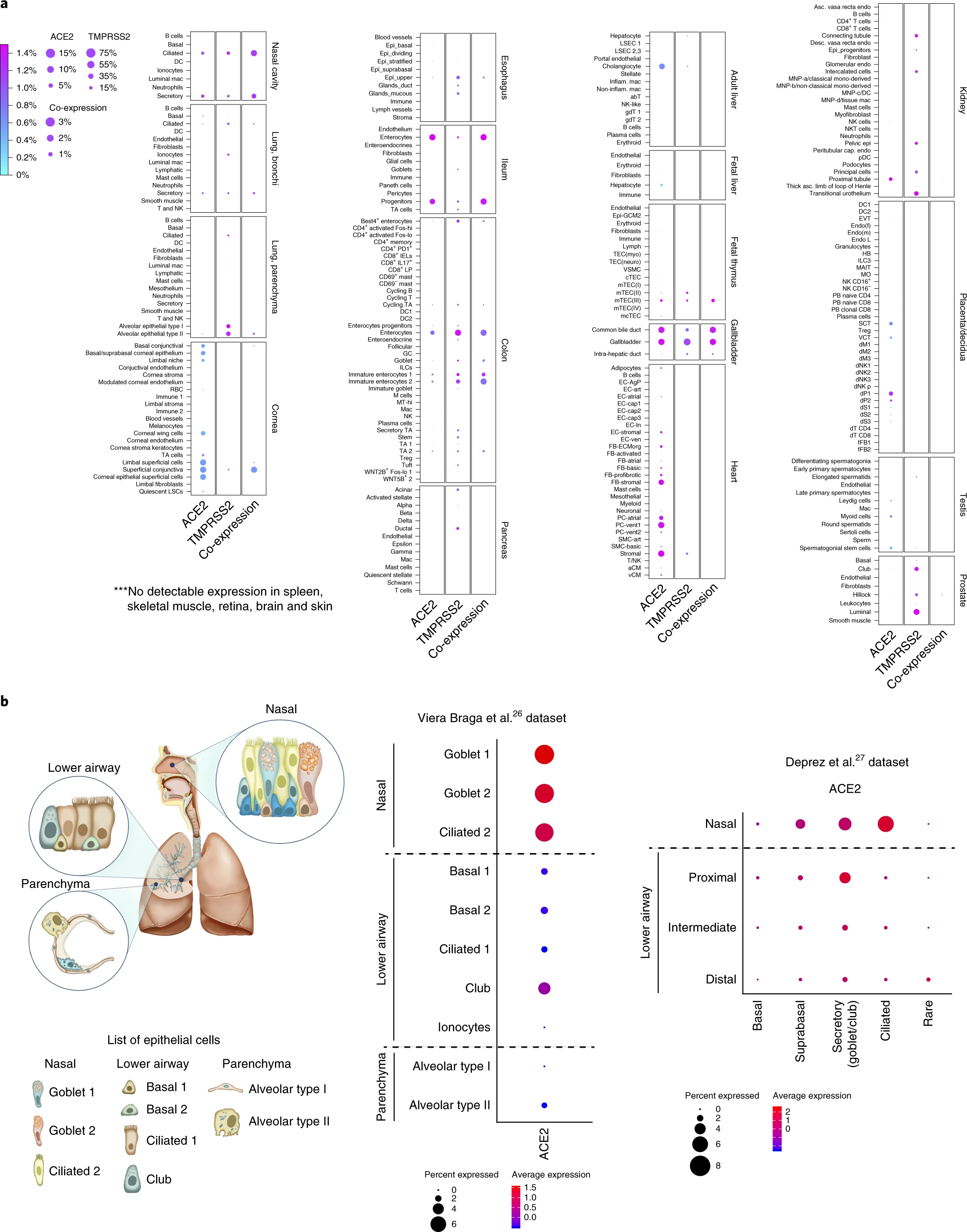{kind=link}
up-regulation on ACE2 expression
- many believe that those who have higher expression of ACE2 or perhaps certain polymorphisms of ACE2 on their cells are at higher risk of severe illness and death although recent studies have failed to demonstrate a significant association with ACE inhibitors or angiotensin II receptor blockers (ARBs) with infection rates or severity of Covid-1927)28)
- ACE2 receptor is not expressed on fetal or placental cells, and is minimally expression in children
- factors which are known to increase ACE2 expression on cells include:
- age
- diabetes
-
- both of which reduce the effect of Ang II on the AT1R which acts to reduce ACE2 expression via lysosomal internalization of ACE2
- ARBs increase ACE2 receptor numbers by 3-5x
- perhaps with genetic polymorphisms of ACE2
- human influenza infection induces broader expression of ACE2 in upper airway epithelial cells
- Covid-19 activated interferon alpha 29)
potential other protein interactions
- co-evolved proteins with ACE2
- ACE2 may have novel protein interactions that are disrupted during SARS-CoV-2 infection30) such as:
- ACE2 has clear connections to coagulation pathway proteins, such as Coagulation Factor V and fibrinogen components FGA, FGB, and FGG, the latter possibly mediated through ACE2 connections to Clusterin (which clears misfolded extracellular proteins) and GPR141 (whose functions are relatively unknown)
- ACE2 also connects to proteins involved in cytokine signaling and immune response (e.g. XCR1, IFNAR2 and TLR8), and to Androgen Receptor (AR)
transmission to other species including pets
- it has been shown that the virus can be transmitted to pets which may then become vectors and reservoirs for the virus, especially ferrets and young cats, while dogs have only low susceptibility, and pigs, chickens, and ducks are not susceptible to SARS-CoV-2 31)
- ferrets and cats have only two amino acid differences in the SARS-CoV-2 spike-contacting regions of ACE2
- ACE2 is mainly expressed in type II pneumocytes and serous epithelial cells of tracheo-bronchial submucosal glands in ferrets but seems to only be replicated in upper airways and not affect the lungs of ferrets
Risk factors for severe disease
genetic
- male
- Blood group O have lower risk (OR 0.65) and blood group A, higher risk (OR 1.45) for severe disease32)
- 5 genes (IFNAR2, TYK2, OAS1, DPP9 and CCR2) appear to be correlated with severe disease according to UK study of 2700 ICU patients
- Neanderthal Chromosome 3 chemokine genes CCR1, CCR2, CCR3, CCR5, CCR9, CXCR6, and XCR1 appear to be a risk for developing severe Covid-19 whilst conferring a 27% reduced risk in HIV 33)
- rare X chromosomal genes producing loss-of-function Toll-like receptor 7 (TLR7) resulting in impaired immune response and reduced type I and type II interferon production appears to markedly increase severity in young men. The highly specific defect in host defense against SARS-CoV-2 and potentially other coronaviruses in these individuals with TLR7 deficiency has similarities with the specific susceptibility to herpes encephalitis in patients with defects in the TLR3 recognition pathway 34)
- rare type I IFN immunodeficiencies such as the AR form of IFNAR1 deficiency35)
co-morbidities
- elderly
- cardiovascular disease
other factors
Prevention
- social distancing
- cough and hand hygiene
- surgical masks for infected persons
- PPE incuding N95 masks for those in close contact:
- environmental cleaning
- vaccination
- unvaccinated people in their 60's had a 60x risk of needing ICU than double vaxed people in their 60's in UK in May-Nov 2021 (ie. Delta variant), and of those in 30's and 40s, the risk was 10-15x more in unvaccinated 39))
- some natural substances can bind the spike protein and potentially reduce severity
Immune response and immunity
- SARS-CoV-2 generates robust antibody responses, including specific IgG, IgA, and IgM.
- seroconversion in infected individuals occurs within 20 days after symptom onset
- it appears that early production of secretory IgA plays an important role and appear to occur prior to specific IgG production and to decline rapidly after a month41)
- the TLR7 pathway is instrumental in the production of type I IFNs in airway epithelial cells
- the SARS-CoV-2 genome contains more ssRNA motifs that could interact with TLR7 than the SARS-CoV genome, indicating that TLR7 signaling might be even more relevant in the pathogenesis of COVID-19 disease
- in comparison with other respiratory viruses, SARS-CoV-2 induces a lower antiviral transcriptional response marked by low type I IFN levels and elevated chemokine expression
- patients with severe COVID-19 exhibit an impaired type I IFN response and a lower viral clearance
- CD4+ and CD8+ T cells play a crucial role in clearing viral infection via the secretion of Granzyme B, a cytotoxic molecule in the nasal cavity but do not seem to do this in the lungs 42)
vaccination
- vaccination appears to produce two main immune responses:
- vaccine-induced humoral response
- provides rapid protection against symptomatic infection by controlling viral replication but this tends to wane over time and may warrant boosters to reduce mild breakthrough infections as it wanes
- vaccinated persons appear to have 5x lower risk of catching Covid-19 43)
- memory immune cells (B cells and T cells)
- 3rd booster dose of mRNA vax significantly further reduces risk of serious illness compared with 2 doses at 5 months since last dose 46)
re-infection
- breakthrough infections are possible as humoral immunity wanes but is generally mild although new variant infections may result in severe infections
multi-dose BCG vaccination
- the Covid-19 vaccines did not work well for type 1 diabetics
- however it was found that multi-dose BCG vaccinations with a particularly potent strain of BCG vaccine may have life long effectiveness against all Covid-19 strains, influenza, RSV
- as the US population were never given an initial BCG vaccination, and normally the full protection for off-target infections takes 2 years, a study using 5-6 doses of a potent strain of BCG vaccination in type 1 diabetics in the US showed 92% efficacy with the early Covid-19 strains 47) and overall 53% efficacy across the 36 month study period PLUS lower rates of viral, bacterial, and fungal infections! 48)
Pathogenesis of illness
asymptomatic nasal carriage
- the virus enters the nasal goblet and ciliated cells and is secreted along with nasal secretions which can then be spread to others primarily by droplet transmission
- the high rates of transmission from asymptomatic infected persons makes control much more difficult and requires testing of all people especially in high risk environments such as aged care facilities 49)
mild URTI/LRTI illness +/- diarrhoea
- infection of nasal cells may result in rhinorrhoea and spread down bronchi to the lung alveolar cells
- this may result in cough, fever and SOB
- even in this mild illness stage a ground glass radiologic appearance of the lungs is often evident suggesting the presence of alveolar fluid
- some will develop silent hypoxia with mild symptoms and this is most likely due to the development of a V/Q shunt whereby pulmonary blood is still provided to alveolar regions with poor oxygen diffusion capacity
- viral particles from the nose will also be ingested and presumably will be taken up by upper oesophageal cells as well as ileal and colonic enterocytes
- this may cause diarrhoea (usually mild), nausea and abdominal pains in some patients
- this may also be a mechanism for fecal-oral transmission
endothelial cell infection and cardiovascular complications
- the ACE2 receptor is also widely expressed on endothelial cells which form an active paracrine, endocrine, and autocrine organ that is indispensable for the regulation of vascular tone and the maintenance of vascular homoeostasis
- induction of apoptosis and pyroptosis might have an important role in endothelial cell injury in patients with COVID-19
- COVID-19-endotheliitis could explain the systemic impaired microcirculatory function in different vascular beds and their clinical sequelae in patients with COVID-1950)
severe disease and CRS
- up to 20% develop severe disease, and 5% become criticall ill most notably with severe pneumonitis / ARDS-like syndrome
- this is thought to occur due to the development of cytokine release syndrome (CRS) and secondary hemophagocytic lymphohistiocytosis (sHLH)
- The efficacy of IL-6–IL-6R antagonists for the treatment of CRS as well as sHLH underscores the central role of IL-6 signaling in the pathophysiology of cytokine-driven hyperinflammatory syndromes
- ARDS results in severe hypoxia due to damage of the alveolar epithelial and endothelial capillary barriers, leading to fluid accumulation, alveolar collapse and reduced gas exchange
- recovery partly relies upon fluid reabsorption and surfactant production which involve metabolic processes performed by the alveolar epithelial cells
cytokine release syndrome (CRS)
- CRS was found to be the major cause of morbidity in patients infected with SARS virus and MERS
- SARS-CoV efficiently infects primary human monocytes and dendritic cells, whereas MERS-CoV infects monocytes and T cells via dipeptidyl peptidase 4 (DPP4)
- it is thought SARS-CoV-2 may function similarly to SARS-CoV in this regard
- betacoronavirus infection of monocytes, macrophages, and dendritic cells results in51):
- dendritic cell dysfunction is thought to lead to defective activation of T cells and resultant T cell apoptosis and exhaustion and lymphopenia.
- their activation and secretion of IL-6 and other inflammatory cytokines
- elevated serum IL-6 increases C reactive protein (CRP) and correlates with respiratory failure, ARDS, and adverse clinical outcomes
- IL-6 can signal through three main pathways:
- classic cis signaling:
- IL-6 binds to membrane-bound IL-6 receptor (mIL-6R) in a complex with gp130;
- downstream signal transduction is mediated by JAKs (Janus kinases) and STAT3 (signal transducer and activator of transcription 3).
- Membrane-bound gp130 is ubiquitously expressed, whereas mIL-6R expression is restricted largely to immune cells.
- Activation of cis signaling results in pleiotropic effects on the acquired immune system (B and T cells) as well as the innate immune system (neutrophils, macrophages, and natural killer (NK) cells), which can contribute to CRS
- trans signaling:
- high circulating concentrations of IL-6 bind to the soluble form of IL-6R (sIL-6R), forming a complex with a gp130 dimer on potentially all cell surfaces.
- The resultant IL-6–sIL-6R–JAK-STAT3 signaling is then activated in cells that do not express mIL-6R, such as endothelial cells.
- This results in a systemic “cytokine storm” involving secretion of vascular endothelial growth factor (VEGF), monocyte chemoattractant protein–1 (MCP-1), IL-8, and additional IL-6, as well as reduced E-cadherin expression on endothelial cells.
- VEGF and reduced E-cadherin expression contribute to vascular permeability and leakage, which participate in the pathophysiology of hypotension and pulmonary dysfunction in ARDS.
- trans presentation
- IL-6 binding to mIL-6R expressed on an immune cell, which forms a complex with gp130 on T helper 17 (TH17) cells, leading to downstream T cell signaling that may be involved in ARDS
- this can be blocked by IL‐6R inhibitors but not by IL‐6 inhibitors which can only suppress only cis and trans signaling
cardiac pathology
- Covid-19 and cardiac arrhythmia risk:
secondary hemophagocytic lymphohistiocytosis (sHLH)
- sHLH is a hyperinflammatory syndrome (aka macrophage activation syndrome) characterized by:
- CRS with elevated serum cytokines
- cytopenias (low blood cell counts)
- high concentrations of ferritin thought to be due to activation of CD163-expressing macrophages which have a role in reticuloendothelial iron signaling
- multiorgan failure
cell death and apotosis induced by the virus
long Covid syndrome
- characterized by symptoms such as fatigue, dysautonomia, pulmonary dysfunction, cognitive disturbances, and others that present within three months following COVID-19 recovery and persist for two months or more (WHO)
- condition is heterogeneous and governed by individual-specific interplays between genetics and environmental exposures
- associations:
- lower levels of morning cortisol
- increased activation of B cells and certain types of T cells
- enhanced antibody responses to the spike protein - suggests persisting viral antigen
- current main hypotheses for Long Covid syndrome:
- persistent Covid-19 infection
- reactivation of latent viruses occurs in a subset of patients, these include HSV, EBV, VZ virus
- autoimmune reaction
- it appears those with certain FOXP4 gene variants have a statistically significant risk association with long COVID, an association found to be independent of FOXP4's previously identified link to severe COVID-19 52)
- chronic inflammation and hypercoagulability
- persistent activation of complement system seems to play a key role in Long Covid
- patients experiencing Long COVID exhibited changes to blood serum proteins indicating activation of the immune system’s complement cascade, altered coagulation, and tissue injury. At the cellular level, Long Covid was linked to aggregates comprising monocytes and platelets. 53)
- reduced serotonin levels due to persistent gut inflammation as a cause of brain fog
- chronic inflammation of the gut via viral RNA-induced type 1 interferons appears to result in reduced absorption of tryptophan and relative depletion of serotonin levels and thus persistent Covid-19 viral presence in the gut is suggested to cause long Covid “brain fog” by depleting serotonin and this reduces vagal nerve impulses back to the brain and resultant reduced activity of the hippocampus - mouse models seem to be able to reverse this effect by stimulating the vagus nerve or by restoring serotonin levels. Serotonin levels may be further reduced by type 1 interferons causing hypercoagulability and thus platelet activation and increased use of serotonin. 54)
- a 2022 pilot study presented at the European Congress of Clinical Microbiology and Infectious Diseases (ECCMID 2022, Lisbon, April 23-26) suggests SARS-CoV-2-mediated vagus nerve dysfunction (VND) could explain some long COVID symptoms, including dysphonia (persistent voice problems), dysphagia (difficulty in swallowing), dizziness, tachycardia (abnormally high heart rate), orthostatic hypotension (low blood pressure) and diarrhea.
- median prior duration of symptoms was 14 months
- 86% had at least 3 VND-related symptoms
- 72% had a positive screen for self-perceived oropharyngeal dysphagia
- 47% had GOR
- 63% showed reduced maximum inspiration pressures, showing weakness of breathing muscles
- 46% had a decrease in diaphragmatic mobility during breathing shown by thoracic ultrasound showing flattened 'diaphragmatic curves'
- 27% displayed alteration of the vagus nerve in the neck shown by ultrasound - including both thickening of the nerve and increased 'echogenicity' indicating inflammation
increased risks of long term illnesses
- 12 month increased burden of disease:
-
- suggests increased burden of AF or CCF is approx 10 per 1000 people while excess PE, Ventricular arrhythmias, AMI are about 5 per 1000 people
-
- lung changes have often persisted at the 2yr mark
- increased risk of new Dx diabetes mainly in those not vaccinated 55)
- increased risk of auto-immune diseases developing 56)
pregnancy
- fortunately it does not seem to have a dramatic impact on pregnant women compared to non-pregnant women with Covid infection, nor to their babies
- in this systematic review of the literature published in July 2020 in The Lancet57):
- ICU admission rate 7% (higher in those with co-morbidities or aged over 35yrs)
- intubation rate 3.4%
- maternal mortality 1%
- pre-term delivery before 37 wks was 22% but mainly medically indicated
therapeutics
- anticoagulants
- propylactic dose anticoagulants reduce Covid clotting complications and ICU admits and death
- individuals using anticoagulation therapy who developed COVID-19 had a 43% lower risk of hospital admission 58)
- Dexamethasone
- the Recovery Trial published in June 2020 showed that 6mg dexamethasone daily for 10 days reduced deaths by 1/3rd for ventilated patients and by 20% for those on oxygen but without need for ventilator care59)
- inhaled steroids
- budesonide
- a UK study published in Aug 2021 appears to show a very significant benefit of using budesonide in those (mainly unvaccinated) over 65yrs, or those over 50yrs with co-morbidities early in their illness as it seems to reduce illness duration by around 3 days howver affect on hospitalisation rates, mechanical ventilation need were not statistically different in each group 60)
- Metadichol®, a nano lipid formulation of long chain alcohols:
- it apparently is a safe, non-toxic product
- inhibits TMPRSS2 (EC50 of 96 ng/ml). It is 270 times more potent than another another well known inhibitor Camostat mesylate, which has EC50 of (26000 ng/ml)
- is also a moderate inhibitor of ACE2 with an EC50 of 31 µg/ml. Moderate inhibition of ACE2 allows it to perform its key functions in the body, yet fend off SARS-COV-2 entry to the cell
- by binding to the Vitamin D receptor (VDR), acts on proteases like Furin and Adam-17, which activate the S-protein spikes for viral spread and pathogenesis in the infected hosts.
- in small studies appears to rapidly clear the virus from infected patients61)
- ultra-high dose vitamin C
- produced a radical improvement in a Melbourne patient in severe sepsis with Covid-19 and seems to have support in animal models
- initial dose of 30 grams of IV sodium ascorbate (vitamin C) over 30 minutes, then a maintenance dose of 30 grams over six and a half hours
- vitamin C and zinc
- appear to increase antibody response 62)
- remdesivir
- in the DisCoVeRy study published Sept 2021, no clinical benefit was observed from the use of remdesivir in patients who were admitted to hospital for COVID-19, were symptomatic for more than 7 days, and required oxygen support.63) Two prior studies reported a faster time to recovery in patients treated with remdesivir, although no difference in mortality was observed overall.
- molnupiravir
- Merck say early results (Oct 2021) in their trials appears to show giving 5 day course of this oral medication within five days of onset of COVID-19 symptoms had about half the rate of hospitalisation and death compared to placebo hence trial was stopped early. Merck say they can make 10 million doses by end of year and US have committed to buying 1.7 million doses if authorised by FDA.
23)
Jeonghwan Youk et al. Three-dimensional human alveolar stem cell culture models reveal infection response to SARS-CoV-2. Cell Stem Cell; 21 Oct 2020; DOI: 10.1016/j.stem.2020.10.004
39)
Intensive Care National Audit and Research Centre (ICNARC
covid19_science.txt · Last modified: 2025/12/17 07:09 by gary1